|
| |
| |
Reprinted from the May 15, 1995, issue of
MODERN HEALTHCARE,
Copyright, Crain Communications Inc., 740 Rush, Chicago, IL 60611 All rights
reserved.
By Sandy Lutz
|
| More for-profit chains court public
hospitals |
Public hospitals and investor-owned hospital chains appear
to be reverse images of each other. One receives tax support; the other pays
taxes. One exists to treat patients who can’t pay for medical care; the
other focuses on generating a profit.
Yet, these images could blur as investor-owned chains seek out public
hospitals for their broadening networks.
“There is a lot of discussion going on between public hospitals and the
for-profits,” said David Hunter, president of the Hunter Group, a St.
Petersburg, Fla.-based consulting firm that specializes in hospital
management. “In some cases, the community will be better off; in some, it
would be better if a community not-for-profit steps up to the plate,” he
said.
But mixing for-profit chains and public hospitals can be explosive.
Witness the sparks this month in Tampa, Fla.
County-owned Tampa General Hospital is in the throes of accusations over
whether its board and former chief executive officer secretly tried to sell
it to the nation’s largest hospital company, Columbia/HCA Healthcare Corp.
Columbia and former Tampa General CEO David Bussone deny any secrecy, saying
their discussion were about managed-care contracts.
However, according to documents released last week, the always
acquisition-minded Columbia did propose a potential joint venture with the
public hospital, modeled after similar deals with private, not-for-profit
hospitals in Florida and Texas.
A letter from Columbia’s Florida President Dan Moen to Tampa General
chairman Frank Fleischer included a draft proposal of how a joint venture
would work (See chart).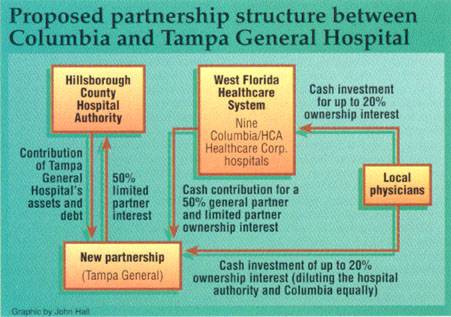
Officials hoped the documents, which include letters exchanged by hospital
board members and Columbia officials, would help settle allegations that the
Nashville, Tenn.-based hospital chain and Bussone worked in secret.
“Every action we chose had prior approval by the (hospital) authority and is
documented in public record,” said Bussone, who now is administrator at
Columbia hospital in Plantation, Fla.
“Like many other non-taxpaying, public-supported facilities, (Tampa General)
is finding it very hard to compete in a managed-care world.” Bussone added.
Ironically, Bussone and two other public hospital CEOs made the cover of
MODERN HEALTHCARE’s Dec. 23/30, 1991, issue for their ability to turn a
profit amid rising charity-care burdens. The story featured Bussone; Ron
Anderson, M.D., of Parkland Memorial Hospital in Dallas; and James C. Pickle
or Erlanger Medical Center in Chattanooga, Tenn.
Favorable for-profits. Tampa General’s situation may not be unique.
With expected cuts in Medicaid and Medicare spending, public hospitals might
begin to look on for-profit chains with new favor.
In the past, investor-owned chains haven’t actively courted public
hospitals, especially ones in urban areas that have large indigent-care
loads. However, the hospital merger and acquisition business has reached
unprecedented levels in the past two years, making the sales of public
hospitals more of a possibility.
Recently, the county hospital in Santa Rosa, Calif., put out a request for
proposals, saying it needed to be part of a network (April 24, p. 92).
Rather than selling to a for-profit chain, public hospitals have been more
likely to privatize themselves by shifting their operations to a new
not-for-profit corporation. In the past, Tampa General had considered such a
privatization, what Bussone said board members often referred to as “the big
P”.
A handful of county and city-owned hospitals have been sold to for-profit
chains in the past. Many are managed by for-profit chains.
Still, the activity to acquire public hospitals seems to be on the rise.
Talking to Columbia. One recent example is Northwest Texas Healthcare
System, a public hospital district in Amarillo that has been talking to
Columbia about a possible purchase.
The hospital district now receives $8.2 million in annual tax support. “What
they have said is that they would eliminate the tax and live up to our
charity-care commitments,” said William Webster, the hospital’s president
and CEO. The hospital spent $21.2 million on charity care in 1994.
|
|
Despite recent discussion with Columbia, Northwest Texas will take time to
analyze all its options. Executive recently hired Nemzoff & Co., Nashville,
to conduct an analysis of the hospital’s options. |
Northwest Texas is profitable, but it’s a freestanding institution that
needs to be part of a managed-care network, Webster said. The hospital
reported net income of $13.8 million on revenues of $129 million in the
fiscal year ended Sept. 30, 1994.
Like most public hospitals in the state, Northwest Texas receives a
significant amount of Medicaid disproportionate-share money, a program that
may end soon if congressional Republicans succeed in moving to a block grant
program. In 1994, Northwest Texas received $12.2 million in
disproportionate-share reimbursement.
The sale of the hospital could open a wide-ranging public discussion in
Amarillo as it has in other locales. Because Northwest Texas is a public
hospital, a possible sale would require an open bidding process and,
perhaps, a voter referendum.
Throwing these matters open to voters can produce the same kind of political
rhetoric of other elections.
That’s the situation in Tarpon Springs, Fla., where a proposal to lease
city-owned Helen Ellis Memorial Hospital to Columbia has been the subject of
a spirited debate.
Unlike other city-owned hospitals, Helen Ellis is not operated by the city
and receives not tax support. It is operated by a private foundation, which
continues to want a deal with Columbia.
The original proposal was a 50-50 venture in which the foundation
contributed the hospital’s assets and Columbia contributed an outpatient
surgery center, home healthcare agency and $14 million in cash. The hospital
was valued at $50 million.
Last month, the city commissioners voted not to set a referendum on leasing
the city-owned facility to Columbia and instructed the hospital board to
look for other partners “with community-based missions” (April 24, p. 4)
One of the commission’s concerns is at the core of these deals: whether a
hospital can serve two masters, the community and shareholders.
“As a limited partner in a for-profit venture, the foundation will have an
incentive to act in the interests of the partnership, which may or may not
coincide with the city’s interests,” the commissioners said. In addition,
the city was worried that with Columbia in control, the city’s best
interests would not longer be paramount in the hospital’s operation.
“Columbia’s principal allegiance must necessarily be to its shareholders,”
commissioners added.
Despite the commission vote, Helen Ellis’ board recently decided to extend a
letter of intent with Columbia until the end of this month, hoping to work
out a deal the city will find agreeable.
“They’re concerned about the size of this company and their takeover
mentality.” Joseph Kiefer, the hospital’s administrator, said about city
officials’ concerns with Columbia.
He still sees Columbia as the best possible choice.
Last year, the board asked for proposals from possible suitors and received
five responses – all but one from investor-owned companies. The lone
not-for-profit was University Community Hospital in Tampa.
Small-town public hospitals haven’t been quite as hesitant to turn to
for-profit chains.
Last year, Troy, Ala., sold its 97-bed Edge Regional Medical Center to
Houston-based Community Health Systems for $14 million.
Twelve years earlier, when newly elected Mayor Jimmy Lunsford proposed
selling the hospital, “I was the biggest scoundrel in town,” he said.
But since then the hospital’s occupancy began ebbing, and efforts to recruit
doctors became harder and harder.
When he proposed selling it in 1994, there was “virtually 100% support” from
the town, he said. |
|